 |
Funded by:
Howard Hughes Medical
Institute
Committee on
Institutional Studies and Research, MSU
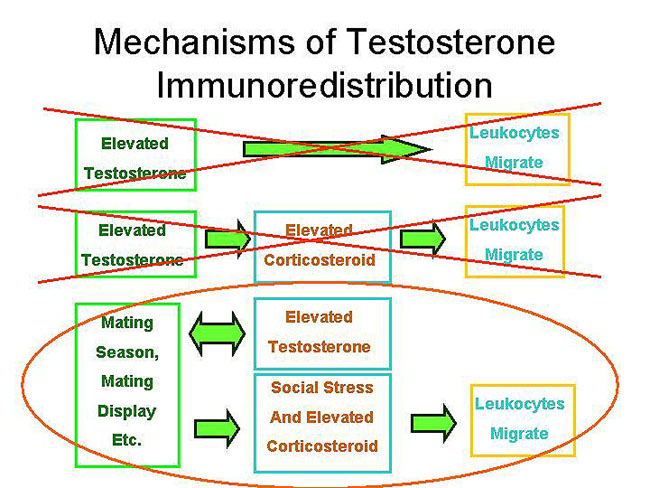
Controversy exists regarding the relationship between immune
function and increased testosterone level, as occurs during mating and
aggressive interactions. A number of researchers have reported
an inverse relationship between testosterone level and immune function
that is mediated by corticosteroid. These data agree with studies
that indicate the existence of trade-offs in energy and nutrient use
between the immune and reproductive systems, particularly during times
of stress. More recent studies suggest, however, that the
decrease in some indicators of immune function in animals with high
testosterone
levels is due to immundoredistribution, rather than
immunosuppression.
According to the immunoredistribution hypothesis, during an
immunochallenge
leukocytes are redistributed to areas of injury or infection for more
effective defense against pathogens. If redistribution does
occur,
then increases in testosterone level may be associated with increased,
rather than decreased, immunocompetence.
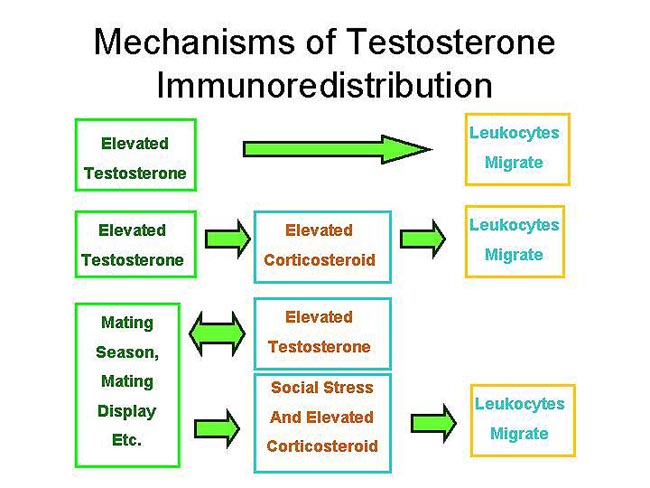
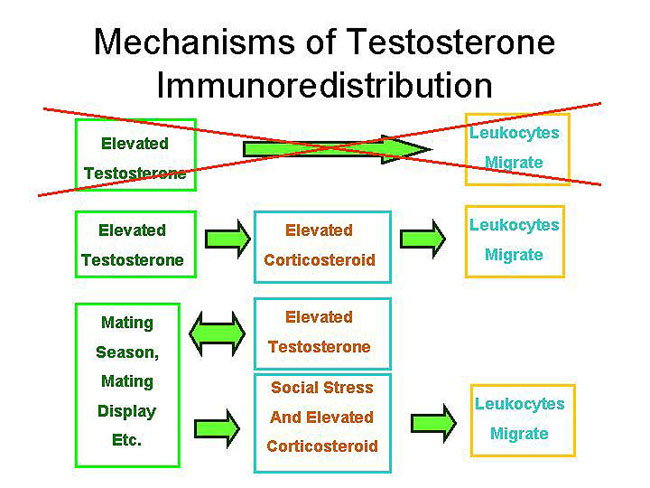
In our initial research we tested the following mechanisms
of action of testosterone:
| |
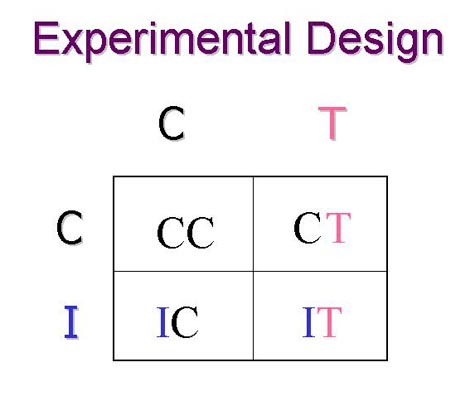 We used a two-by-two design with testosterone level (T) and immunochallenge (I) as the two treatment variables. Corresponding controls (C) were established. The result was four groups of adult male white-footed mice. |
 |
 |
 |
 |
Richard Blalock conducts a hemaglutination test (top left) for humoral immune responsiveness; Marshall Welch and Maninder Virk obtain core blood by heart puncture (middle right); and peripheral blood is obtained from the retro-orbital sinus (far right); Lee Webb and Brandon Kellie conduct radio-immuno assays to determine testosterone and corticosterone levels (middle left).
 |
|
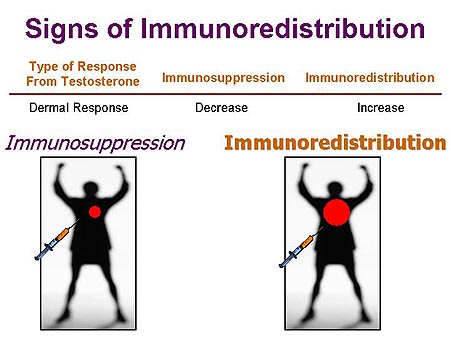
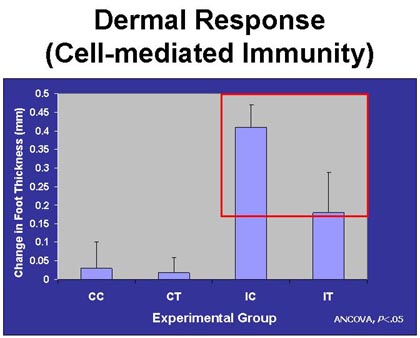
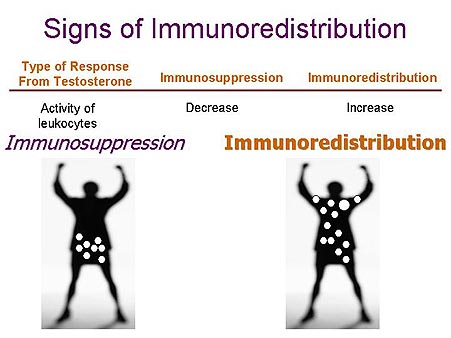
| If testosterone causes immunosuppression, then a small dermal response was expected after injection with phytohemagglutinen. If immunoredistribution results, then a large dermal response was expected. | Immunochallenged animals without testosterone (IC) had a much greater dermal response than immunochallenged animals with elevated testosterone levels (IT). These results supported the immunosuppression hypothesis. |
 |
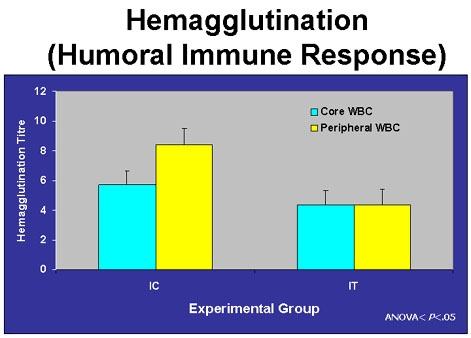 |
| If testosterone causes immunosuppression, then we expected the activity of leukocytes to be suppressed. The opposite result was expected if testosterone stimulates immunoredistribution. | The responsiveness of the humoral branch of the immune system was reduced, especially in the peripheral blood, in animals with elevated levels of testosterone (IT) compared with animals control animals (IC). These results supported the immunosuppression hypothesis. |
 |
|
CONCLUSION 1: Testosterone does not cause leukocytes to migrate to peripheral areas of the body during an immunochallenge. |
 Testosterone had a suppressive effect on corticosterone. |
 Lee and Brandon conduct radio-immuno assays to determine blood concentrations of testosterone and corticosterone. |
 |
|